[WK] Trypsin is a pancreatic extract from pigs or cows that is used in digestion. In polio vaccine production it was used historically in three stages..
For classical polio vaccine production using individual monkeys, trypsin is used in three distinct stages:
First Stage a live monkey would be infused with trypsin to dissolve the binding materials inside its kidneys and allow the cells to flow out into a flask.
Second Stage when the cells were grown out in Modified Eagle medium, trypsin was used to dissolve any binding materials and allow the cells to grow in a smooth monolayer.
Third Stage in the final stage, after a monolayer of cells are grown out, trypsin is added to allow the polio viruses to infect the cells by modification of the cell membrane and potentially the vaccine strain virus also.
75-85% of the porcine trypsin used in vaccine production in the EU and US is contaminated with circoviruses that replicate in a way reminiscent of auto-immune disease outbreaks. Trypsin also allows any other monkey viruses present in the kidney cells to access them like polio viruses, SV-40, for example in Salk IPV of the 1950s. Simian Immunodeficiency Viruses, Epstein Barr Virus, Cytomegaloviruses and Simian Agent 8 (HSV-1 & 2, genital herpes) were just a few of the 20+ other viruses carried by the monkeys used in Sabin vaccine production that used all three stages of trypsin.
Julius Youngner, Salk’s assistant, discovered trypsin allowed polio to infect monkey kidney cells, a plentiful source for massive vaccine production.
Salk made the assumption, based on this history, that injections containing live polio viruses would not cause systemic infections (flu, fevers, excretion in the stool), and rarely cause paralysis if the injected virus accessed a nerve cell and moved backwards into the spinal cord (retrograde atonal transport).
But trypsin changed the nature of injected viruses, and according to Langmuir, caused multiple systemic infections per his June 30, 1955 Memo entitled “Poliomyelitis Vaccine Assessment.” That appears poignant to today’s AFM outbreak where synthetic trypsin (Medium 199) is injected with the vaccine viruses.
Did trypsinization cause retrograde axonal transport that leads to injection limb paralysis, which was similar to the Salk outbreaks in California and Boston? What can you tell us about any victims of those outbreaks?
Historically, Salk expected retrograde atonal transport would result if a live injected virus accessed a nerve and made its way back to the spinal cord, which would result in injection limb or opposite injected limb paralysis as the first sign of poliomyelitis. Note that paralytic polio caused by wild virus was systemic and classically began in one of the lower legs, then the other and moved up the body, thus it was diagnosed as asymmetric, ascending flaccid paralysis.
It is important to emphasize that most of the victims were family members, or classmates, of the recipient of the vaccine who might never be paralyzed but the recipient’s systemic infections could paralyze people in close personal contact with them. The Vaccine Injury Table recognizes the phenomenon.
Most of the victims of the polio virus in Salk Vaccine (which was also contaminated with SV-40) were contacts of the recipient. These victims’ paralysis arose from the systemic infection of the recipient – not retrograde axonal transport that involved either the injection itself or spread from the recipients to simultaneously M-199 injected Placebos in the Francis Field Trial.
Fathers acquired polio from Salk vaccine in the Boston epidemic at a higher rate than Mothers of injected children – a unique anomaly that is consistent with the first case of AFM in the 29-year-old father of an immunized child.
BOSTON – Summer of 1955 – after “The Cutter Incident.”
The Parke Davis (Lot 1018) rework in Boston and Wisconsin involved over 7000 cases of poliomyelitis. Over 400,000 cases may have occurred in Massachusetts alone, including the non-paralytic events. All BOSTON Hospitals shut down non-emergency services to care for victims of the Salk vaccine.
The Massachusetts Medical Society dropped recommendation of Salk vaccine, but Joe Smadel, of Walter Reed Army Institute of Medical Research, and Alexander Langmuir, of CDC, touted to the media the vaccine was safe.
The epidemic in Boston arose from reworked, multiple formalin-treated vaccines that caused injection limb paralysis and systemic infections as late as 90 days after injection (the Francis Field Trial only considered cases in Recipients up to 14 days after injection and disregarded them all as caused by wild polio viruses – after all the Placebos acquired polio at twice the rate of Recipients). In Boston Langmuir “epidemiologically eliminated” all cases of polio not arising within 30 days – a false premise that sold the vaccine to the press.
[CJF note: Formalin is a colorless solution of formaldehyde in water, used chiefly as a preservative for biological specimens. (Online Dictionary)]
Subsequent studies showed the formalin plasticized proteins around the live viruses, which resulted in “time released polio.”
CALIFORNIA – THE CUTTER INCIDENT – was actually made vaccine.
The California outbreak occurred the week after licensure and is referred to as The Cutter Incidentwhere it was first recognized that the vaccine caused twice as many cases of polio in personal contacts of the recipients than it did in the recipients of the vaccine. Family members could be paralyzed by a child recipient who remained healthy.
The Cutter Incident has the same rate of reaction as seen in the Francis Field Trial of the Salk vaccine; twice as many personal classroom contacts came down with polio as compared to direct recipients.
Since Salk counted all cases of polio in recipients as caused by wild polio and twice as many classmates came down with polio, he considered the vaccine “effective.” Salk vaccine was never tested for safety in that Field Trial.
Lilly and Parke Davis were the two manufacturers that inactivated polio vaccine for the Francis Field Trial.
It is well known, but not published, that the vaccine in the Cutter Incident was actually produced by Lilly. Cutter was a scapegoat. The reaction rates in Cutter Incident and Francis Field Trial were nearly identical.
Did I mention that Francis was also under military control and actually formulated the Type1 Mahoney strain in 1941 while working for the Rockefeller Foundation?
The vaccine medical literature lists a vaccine incident the CDC blames on Cutter Labs? What can you tell us about that, please?
[WK] That was Lilly vaccine distributed by Cutter, a small firm in California. Cutter was a scapegoat and the reaction rate in Cutter matched the reactions seen in the Francis Field Trial. Lilly also made vaccine for that Francis Field Trial.Most of the 78 cases of polio caused in Cutter IPV recipients arose within 14 days followed by 200+ contact polio cases within 14 days of the recipient’s reactions, essentially the same rate of polio as in the Francis Field Trials.
Is it true there never was a Cutter Labs incident but that it was a press campaign run for the military by a CDC employee, who was Dr. Alexander Langmuir, CDC Chief Epidemiologist for 21 years often referred to as the “Father of CDCs Epidemiological intelligence Service”?
[WK] Langmuir was assigned to the Communicable Disease Center in Atlanta, in 1952, to thwart the expected bioterrorism threat by North Korea and was placed in charge of the cover-up of the Salk vaccine problem at the time of the outbreak in Cutter. He did a great job; if anyone discovered Lilly actually made the vaccine everyone would have known the Francis Field Trial was “Fake Medicine,” but great epidemiology.Keep in mind that Public Health and epidemiology focus only on the public health, and tend to totally disregard individual victims.
That should end. An NTSB-style group should be charged with evaluation of individual injuries, just as NTSB investigates FAA originated air disasters.
What do you know about the Francis Field Trial, which used Lilly and Parke Davis supplied vaccines, where all cases of polio in recipients were blamed on wild viruses?
[WK] Briefly, Lilly inactivated the 300 series Lots and Parke Davis the 500 series batches in the Francis Field Trial. The two companies did not produce the original lots but inactivated vaccines prepared in Canada using M199 instead of trypsin. Connaught Laboratories produced the original batches using M-199 instead of trypsin to avoid contamination of the vaccine with then unknown circoviruses, which were suspected but not yet identified.The M199 was injected into the Placebo group who were the close personal contacts and First and Third Grade classmates of the Recipients of the actual vaccine. The Placebos were paralyzed at over twice the rate of Recipients injected with a semi-inactivated vaccine…just like in the Cutter Incident. Salk assumed the injected vaccine could not cause polio, in general, and interpreted the results to mean that since Recipients acquired wild polio at half the rate of the Placebos, the vaccine was “effective”!
Salk never tested the vaccine for safety; he theorized it was nearly impossible to get polio from injection of live polio viruses.
Only after Langmuir concocted the Cutter Incident epidemiology did the Surgeon General declare the vaccine safe. Then came the Boston epidemic where physicians were subject to criminal penalties for fingering Salk vaccine as its cause.
The Francis Field Trial conducted in 1954, involved 1,873,483 children. It was an Efficacy ONLY study because Salk and Francis assumed that injection of live polio could not cause polio when the trial was conducted. Is it true the efficacy of preventing paralytic poliomyelitis was 70.0 percent?
Do you know how many children actually contracted polio during that field trial?
[WK] Let me send you Salk’s graph for inclusion here. Salk vaccine was only “efficient” in causing polio in both Recipients and their close personal “Placebo” contacts during the Field Trial. If you cause twice as much polio in Contacts of Recipients as you do in Recipients by injecting live polio viruses, it is not proof of “Effective,” it is proof of a bad vaccine.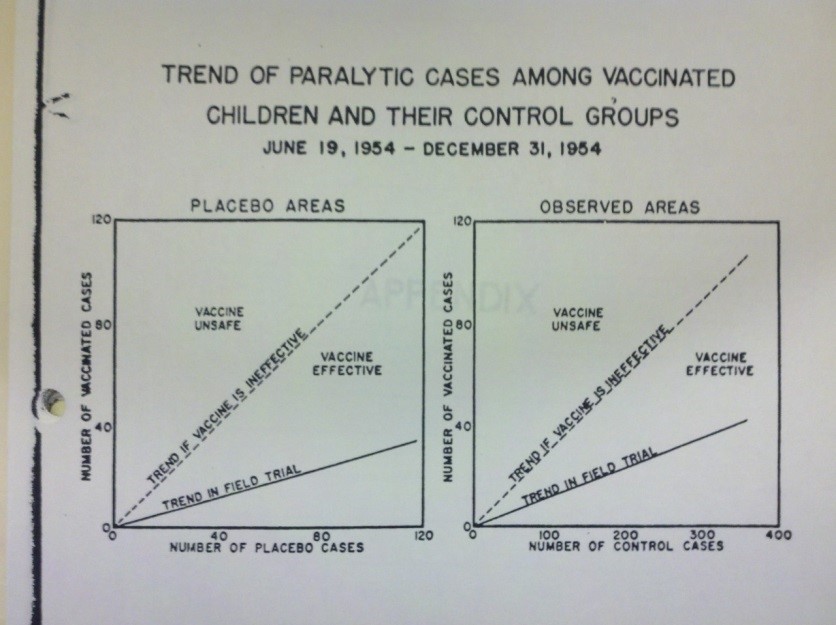 [WK] It took several months to write the report; the third round of immunizations is telling since they occurred in December 1954 when no wild polio existed. But the question is not appropriate since the virus spread from both the Recipients and Placebos to their family and surrounding community. Under the Salk-CDC-Langmuir disinformation protocol the more people who acquired polio in the community via injection with the “vaccine,” the more “effective” the vaccine appeared. GREAT “Epidemiology”; Bogus Science!
[WK] It took several months to write the report; the third round of immunizations is telling since they occurred in December 1954 when no wild polio existed. But the question is not appropriate since the virus spread from both the Recipients and Placebos to their family and surrounding community. Under the Salk-CDC-Langmuir disinformation protocol the more people who acquired polio in the community via injection with the “vaccine,” the more “effective” the vaccine appeared. GREAT “Epidemiology”; Bogus Science!
Is it true that modern new vaccines are tested using many of the methods of the Francis Polio Field Trial? Why is that?
No, not true. The Francis Field Trial is CDC’s Gold Standard, which current vaccines are not required to meet. Nonetheless, current licensing still uses unfounded assumptions, time limitations, and specious arguments tor justification in licensing. It’s a lot cheaper, and since FDA blocks use of available technology to verify vaccine reactions, they can get away with it.
Why did the U.S. military finance the Francis Field Trial in the 1940s-‘50s?
[WK] In 1945 [President] Eisenhower, as Supreme Allied Commander, authorized a “War on Polio.” Polio in North Africa had killed many troops, but did not infect the native population.Major Albert Sabin (Sabin OPV) and John Paul (Johns Hopkins) were dispatched there to obtain the Type-2 MEF strain that was brought back to the US where Type2 polio was not a problem. MEF stands for Middle Eastern Forces.
Enders, at Boston Children’s Hospital, was working on a measles vaccine for the military when he discovered the trypsinization trick that allowed polio to grow in human foreskins and mass produce vaccines.
VA hospitals were filled at the time; polio was primarily a disease of infants, but all boys were subject to the draft. It was best to assure their immunizations took place before the military had to care and pay for reactions to vaccines on induction.
Does that prove the relationship of the military and the CDC over the years and what some contend that the U.S. military spearheads new vaccine production? Why is military vaccine safety data not available to the public?
The public is not allowed to have any vaccine safety data or scientific tests for vaccine reactions.
The military desires future soldiers free from both the diseases and reactions to vaccines. The fundamental design of many vaccines containing multiple biologicals (MMR, DTP, Type-2 polio from North Africa) in a single dose challenges the future recruit, as a child, to multiple contagions expected in boot camp or deployment. Elimination of vaccine reactors, as children, precludes care for them as soldiers.
The military recognizes that no vaccines are “safe” and “free of harmful effects” to millions of users. “Putting Children First” thus eliminates any vaccine harmful effect in future recruits – by process of eliminating the recruit in childhood.
Has vaccinating children during childhood become a military self-serving agenda, since at one time military recruits were coming down with childhood diseases that kept them out of service and in military hospitals?
[WK] Measles was a big problem in boot camps during World Wars 1&2. That’s why the military financed Enders research in Boston. 500,000,000 cases of measles in the civilian population was not a problem in the 1950s because the fatal complications could be treated with penicillin. The military has been in the immunization business since the Revolutionary War when smallpox spread by the British decimated the Continental Army and caused the defeat in the Battle of Quebec.Also, the military wants communities around bases free of infectious diseases like Hepatitis-B, which traditionally appeared only in prostitutes and IV drug users, but is now given to all newborns within 12 hours of birth.
One can almost predict the military’s future war plans based on the forced immunization programs in California, Australia and India…marshaling areas for protection of the oil in the South China Sea?
Is it true no safety testing was ever conducted before using those vaccines?
I’ve heard the military ran the Francis Field Trial on the premise that the vaccine was ‘safe’ if it caused less than one case of polio per thousand injections.
[WK] Jonas Salk, Thomas Francis, Alexander Langmuir, Nobel Laureate John Enders and notably Sam Katz, a Fellow in Enders Lab in the mid ’50s who knew of all the problems caused by Salk vaccine in Boston and later became the Chairman of the Infectious Disease Committee of the American Academy of Pediatrics and Editor of the Redbook, all were controlled through a secret group run out of Walter Reed Army Institute of Research.One reaction per thousand reflects the reaction rate to infection with wild polio. The one in a thousand reaction rate is published as acceptable by an FDA Committee, led by Saul Krugmann (Westbrook School/Hep-b), and dominated by military associated, ostensibly civilian, physicians. See The Federal Register April 15, 1980.
Thus, that reaction rate should be considered acceptable to the military for all vaccines for U.S. children.
Problematically, no children need protection against poliomyelitis now – unless, of course, there are plans to “stage” them in India.
Supposedly, Dr. Langmuir was critical of flu vaccines. Are you aware of the supposed comment he made, that said, “I would not take the flu vaccine. My wife does not take the flu vaccine. No one should take the flu vaccine, and in fact, when I was head of the CDC, I wanted to make that as a public statement and I refused to that you should take the flu vaccine. That’s why I’m now professor at Harvard.” … Alexander Langmuir, former Chief Epidemiologist for the CDC
[WK] He is a smart man. I thought that was a quote from President Trump.Jonas Salk often said polio vaccine was easier to make than flu vaccine. In the early 1950s, VA Hospitals were full of victims of the flu vaccine made by Salk and Francis.
So I can understand why Langmuir would not take Salk’s flu vaccine and oversaw the human experimentation of Salk polio vaccine on children, since the military financed it better to experiment in children not able to get into the overcrowded VA Hospitals.
Walter, can you please comment on the following story about a baby boy, who contracted polio from a vaccine when he was given the oral polio vaccine at four months in 1990, as documented in the article “David Salamone, who contracted polio from vaccine and helped spur changes in U.S. immunization policy, dies at 28”?
[WK] I was aware in the vaccine court litigation that a few cases of polio from Salk vaccine had been filed.I also know of a case in Italy where the doctor published a paper in the Journal of the Royal Society of Medicine, titled “Vaccine-derived poliomyelitis and postpolio syndrome: an Italian Cutter Incident” JRSM Open. 2014 Jan; 5(1): 2042533313511241.Published online 2014 Jan 7. doi: [10.1177/2042533313511241] PMCID: PMC4012681, PMID: 25057364 Elena Angela Lusi1 and Paolo Guarascio2
This deals with a 1960s case of polio following a child’s second Salk Immunization. It also demonstrates how logical, scientific analyses and deductions can prove a case of polio 50 years after the fact. I did contact Dr. Lusi, the lead author, to correct her on the fact that Cutter did not really make the Cutter Incident vaccine. I have assisted Dr. Lusi during the interim in the presentation of papers related to her discovery of a giant retroviral cored virus in humans. Dr. Lusi has named it a Retro-Giant virus. My impression is that it may represent what I call “The Temin Mechanism,” which Howard Temin described in the last illustration during his 1975 Nobel Lecture: the agent inside cells that interacts with benign viruses and converts them to carcinogenic ones. ALV (Avian Leukoma Virus) morphed to ASV (Avian Sarcoma Virus) after interactions within a cell; or it could be something closer to LUCA (the Last Universal Common Ancestor) that is currently known.
My later review of the thousands of documents produced revealed the Cutter vaccine and Field Trial vaccine both came from Lilly. Dr. Alexander Langmuir’s job for CDC was to encapsulate reactions to polio vaccine in a box and deny any that did not comply with his imaginative restrictions. Langmuir, by definition, was not a scientist/clinician; he was a bio-warfare intelligence officer working for the U.S. military that wanted a polio vaccine and none of the six-rear old “soldiers to be” susceptible to polio.
Alexander Langmuir epidemiologically defined VAPP as needing to arise within 30 days of vaccine administration, although Field Trial cases of paralysis arose as much as 40-50 days after recipients got the vaccine but it was blamed on wild polio. Salk assumes the injected vaccine could cause polio in recipients within 14 days, but clumped that group into the vaccine “effectivity” mantra, not as reactions, and under his theory, not able to spread polio to contacts.
Salk vaccine could cause polio after the third immunization via live viruses in it directly accessing the peripheral nerves, thus igniting a backfire to the spinal nerves down the nerve routes even if the recipient had antibodies to polio from prior immunizations.
Remember the Francis “Faked” Field Trial is now the Gold Standard of FDA. Therein is the flaw of our vaccine program: 60 years of fraud threatens thousands of egos.
The use of military-originated-epidemiology, as opposed to clinical medicine evaluation of vaccine reactions, is synonymous with a system of non-safety predicated on a military Standard of Vaccine Acceptability.
Walter, do you have a live link to the following article you wrote?
[Kyle, W.S. 1992. Simian retroviruses, poliovaccine, and origin of AIDS. The Lancet 339: 600-601.]
[WK] It should be in PubMed, but it is hard to find. The defense to that premise has been that SIV will not infect monkey kidney cells, which I now know to be bogus for three reasons:First: polio viruses will not infect the monkey kidney cells used to make the vaccine, either.
Second: Trypsin is needed to induce infection of monkey kidney cells by polioviruses, which would also permit the infection by any latent monkey viruses.
Third: The apparently reference the third stage of polio production after a monolayer is grown out, but during the second stage any latent virus in the blood of the monkey could access and replicate by invasion during cell division – the s-stage – while the monolayer is being “grown”.
Can Transverse myelitis, the condition the vaccine gave the boy, is something that vaccines have been linked to since the 1920s be part of the current AFM?
[WK] I do not believe any diagnosis by physicians since the time Sam Katz took over the Infectious Disease Committee of the American Academy of Pediatrics and published the Redbook. Katz was a brilliant student, chosen by the military at a young age (Charles Janeway at Harvard), and steered into pediatrics during the post-war baby boom. Katz worked in Enders Lab in 1955-‘56 and knew well that the Salk vaccine caused the polio epidemic in Boston, but did he add that factoid to the Vaccine Injury Table – NO – Katz apparently owed allegiance to the military.How did the new AFM classification come from the EV-D68, an enterovirus?
[WK] Similar waves occurred in 2014 and 2016, and scientists have fingered a relative of the poliovirus, called enterovirus D68 (EV-D68), as a possible culprit. EV-D68 is 80% homologous to the Type-1 Mahoney strain of polio vaccine virus. Francis mixed three specimens during an outbreak of polio in 1941 while working for the Rockefeller Foundation and EV-D68 falls within the range of sequences expected from Mahoney Type, considering the use of trypsin/M-199 in production of the current Salk IPV.Vaccinations are political decisions rather than medical. Is it true current vaccines have microchips in them?
[WK] If true, comments about vaccines’ ramifications as the etiology of diseases in the body, especially inducing chronic old-age-type diseases in very young children, is the trend now.I have never actually heard of that suspicion.
What role does fear mongering encouraged by the CDC regarding vaccines, especially the flu vaccine, play in the acceptance of vaccines in general?
Considering what Cochrane researchers concluded, what is your opinion regarding flu vaccines, which are extremely problematic as per claims made to the Vaccine Court, but given to 6-month-old infants and how those multivalent [4 actives] flu vaccines can impact a child’s mitochondria?
[WK] What the Cochrane researchers actually concluded, however, was that their findings “seem to discourage the utilization of vaccination against influenza in healthy adults as a routine public health measure” (emphasis added). Furthermore, given the known serious harms associated with specific flu vaccines, and the CDC’s recommendation that infants as young as six months get a flu shot despite an alarming lack of safety studies for children under two, “large-scale studies assessing important outcomes and directly comparing vaccine types are urgently required.”End of Interview
As an afterthought, even though I didn’t ask Attorney Kyle’s opinions about aluminum adjuvants in vaccines, I’d like readers to know about the recently-published Spanish research paper “Cognition and behavior in sheep repetitively inoculated with aluminum adjuvant-containing vaccines or aluminum adjuvant only” appearing in Pharmacological Research November 3, 2018 wherein 14 researchers agreed
Aluminum (Al)-containing vaccines are common in sheep management and they have been associated with the Autoimmune/inflammatory Syndrome Induced by Adjuvants (ASIA syndrome).
[….]This study is the first to describe behavioral changes in sheep after having received repetitive injections of Al-containing products, explaining some of the clinical signs observed in ovine ASIA syndrome. (Source: Science Direct)
If behavioral changes occurred in sheep, what do such aluminum-adjuvated vaccines do to infants, toddlers, teens, adults and senior citizens? Can the accumulation of aluminum in the brain from mandatory vaccine schedules be contributing to the violent anti-social behavior occurring at all levels in the USA?
According to the U.S. CDC, the following vaccines contain aluminum adjuvants:
Anthrax, DT, DTaP (Daptacel), DTaP (Infanrix), DTaP-IPV (Kinrix), DTaP-IPV (Quadracel), DTaP-HepB-IPV (Pediarix), DTaP –IPV/Hib (Pentacel), Hep A (Havrix), Hep A (Vaqta), Hep B (Engerix-B), Hep B (Recombivax), HepA/Hep B (Twinrix), HIB (PedvaxHIB), HPV (Gardasil 9), Japanese encephalitis (Ixiaro), MenB (Bexsero, Trumenba), Pneumococcal (Prevnar 13), Td (Tenivac), Td (Mass Biologics), Tdap (Adacel), Tdap (Boostrix
in one or more formulae
… of the following: amorphous aluminum hydroxyphosphate sulfate (AAHS), aluminum hydroxide, aluminum phosphate, potassium aluminum sulfate (Alum).
Some vaccines have more than one formulation of aluminum, thereby compounding not only neurological effects of aluminum but ‘complicit’ in every “syndrome” medical science somehow can’t figure out.
Lastly, I think, and suggest, every person’s medical records by law mandatorily must record in detail each vaccine he/she receives, the date, manufacturer and lot number of each vaccine, as that information has to be considered in the “cause and effect” database for whatever physiological condition a person contracts that ultimately will prove vaccines are responsible for all supposed “idiopathic” diseases. Attorney Kyle’s interview proves the need to avoid false data sets.
Notes:
[1] https://www.cdc.gov/acute-flaccid-myelitis/afm-surveillance.html accessed 11/12/18Resource:
Vaccination Voodoo, What YOU Don’t Know About Vaccines
https://www.amazon.com/Vaccination-Voodoo-What-About-Vaccines/dp/1484923820
Catherine J Frompovich (website) is a retired natural nutritionist who earned advanced degrees in Nutrition and Holistic Health Sciences, Certification in Orthomolecular Theory and Practice plus Paralegal Studies. Her work has been published in national and airline magazines since the early 1980s. Catherine authored numerous books on health issues along with co-authoring papers and monographs with physicians, nurses, and holistic healthcare professionals. She has been a consumer healthcare researcher 35 years and counting.
Catherine’s latest book, published October 4, 2013, is Vaccination Voodoo, What YOU Don’t Know About Vaccines, available on Amazon.com.
Her 2012 book A Cancer Answer, Holistic BREAST Cancer Management, A Guide to Effective & Non-Toxic Treatments, is available on Amazon.com and as a Kindle eBook.
Two of Catherine’s more recent books on Amazon.com are Our Chemical Lives And The Hijacking Of Our DNA, A Probe Into What’s Probably Making Us Sick (2009) and Lord, How Can I Make It Through Grieving My Loss, An Inspirational Guide Through the Grieving Process (2008)
Catherine’s NEW book: Eat To Beat Disease, Foods Medicinal Qualities ©2016 Catherine J Frompovich is now available.
Courtesy of Activist Post

Your Daily Briefing:
Fight Online Censorship!
Get the news Google and Facebook don't want you to see: Sign up for DC Dirty Laundry's daily briefing and do your own thinking!